Suffering of body-consciousness is universal,
Caused by desire for existence / nonexistence of “I” and “self”,
Transcendence of suffering is possible,
On the path of true Practice-Insight-Wisdom-Compassion.
(Siddhartha Gautama) [1]
Transformations of psychopathology
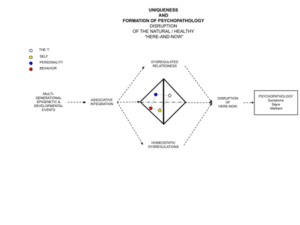
Psychopathology is a facet of uniqueness and, historically, has often been conceptualized as a “biopsychosocial” problem (disorder) involving one’s (i) biophysicality (BODY, neurobehavioral circuits); (ii) psychology (CONSCIOUSNESS, mind, personality, self, subjectivity) and (iii) social (interpersonal, relational) interactions (PERSON) and stressors (LOCATION, challenges, adversity, trauma). Psychopathology evolves and fluctuates (p-i-states) within the four registers of one’s uniqueness as a composite (syndrome) of particular symptoms, signs and markers and can be mitigated by natural life events (age, learning, lifestyle, relational) or modified (cured) by specialized treatments.
Most broadly, transformations of psychopathology, as an aspect of one’s uniqueness, are embedded in an exploration and analysis of how one’s uniqueness and psychopathology interact and reflect each other (Analysis of Uniqueness) and involve (i) changes of the spatiotemporal formation of psychopathological i-states (p-i-states); (ii) changes in the relative and / or perspectival position (subjective, interpersonal and academic) of psychopathological i-states (p-i-states) among other i-states of one’s uniqueness and (iii) changes in the p-i-states’ disruptive relation to health (adaptation, actualization, realization) and resilience. Accordingly, psychopathology can alternate between being expressed as symptoms, signs or markers, based on its etiology (spatiotemporal formation), type (relative / perspectival position) and severity (disruptive relation to health).
Changes in the spatiotemporal formation
Spatiotemporal formation of psychopathological i-states (p-i-states) is based on pathogenic intergenerational epigenetics[2] and compromised progression of associative integration[3] resulting in recurrent patterns of disruptions of the relevant[4] aspects of the here-and-now deemed to be psychopathological (symptoms, signs, markers), subjectively, interpersonally, academically. Spatiotemporal formation of psychopathology involves vulnerabilities of (i) the formation / positionality of the “I”; (ii) homeostatic regulation and (iii) intersubjective relatedness (see Graph P-1 and Graph RV below).
Graph P-1 Formation of Psychopathology
Intergenerational epigenetics can be modified by geopolitical, societal, community and family level interventions focused on prevention and amelioration of stressors, adversities and trauma (natural, geopolitical, societal, biophysical, relational and experiential) across multiple generations of families, parents and children (see other posts).
Associative integration can be improved by direct interventions (health, education) in the maturational, developmental and learning-based neurocognitive processes across all levels of one’s functioning (neurocognitive maturation, learning, memory, self/other representation, “executive” functions, behavior).
Formation / positionality of the “I” is routinely transformed, moment after moment, by changes in the degree of insight (pre-reflective, conscious), mode (sensoriaffective, sensorimotor, ideational, communicative), spatiotemporal position (here-now, dis-associative) and / or form (rigid, multifaceted, transcendent, formless)[5].
At the level of actual psychopathology, homeostatic dysregulations are typically treated by complex interventions (medical, behavioral, life style, psychotherapy) within multiple facets of one’s biophysical functioning – activation (arousal, constraint), negative valence systems (NVS) (distress, pain, fear, anger, anxiety), positive valence systems (PVS) (pleasure, incentive / approach, affiliation, attachment, joy / happiness) and neurocognitive integration (NI) (attention / memory / language cohesion, congruence vs dissociation, psychoticism) (see Volume I, Section 2.4.1) whereas relatedness can be improved by transformative explorations (education, psychotherapy, psychoanalysis, insight) of intersubjective ipsocentricity / allocentricity, autonomy / agency, otherness / alterity, patterns of attachment / affiliation and appraisal of self and others) (see other posts) .
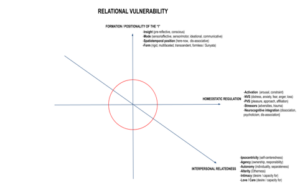
Graph RV Relational Vulnerability
Changes of the relative / perspectival position
Psychopathology (p-i-state) is a disruption of the natural / expected / normative here-now. It is a disruptive i-state formed within a particular region of the four registers of one’s uniqueness (BLCP tetrahedron) (Graph P-2 below).
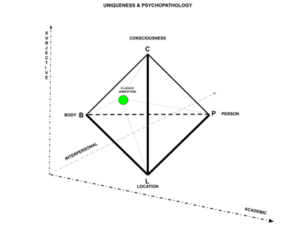
Graph P-2 Psychopathological i-state (p-i-state, disruption) within the BLCP tetrahedron
The relative position of psychopathological p-i-state within the BLCP tetrahedron manifests the relative contribution (participation) of one’s BODY (biophysicality, appearance, behavior), LOCATION (sensory / semantic space), CONSCIOUSNESS (sensations, awareness, ideation) and the PERSON (interpersonal / societal markers) in the formation of symptoms, signs and markers of psychopathology as a disruption of the here-and-now. (Sections 1.1.2; 1.1.5 above).
The perspectival position of a p-i-state refers to a two-step process leading to the determination (interpretation) whether an i-state is experienced (symptom), perceived (sign) or identified (marker) as (i) a disruption and (ii) a manifestation of psychopathology, subjectively, interpersonally and academically.
Most manifestations of psychopathology are a composite (syndrome) of particular symptoms, signs and markers, some may involve, or are actually predicated on, an absence of (or incongruence between) the subjective and / or the interpersonal aspects (lack of awareness, differences in perception / interpretation, secrets, deception).
Changes in the relative / perspectival position of psychopathology involve (i) changes in how symptoms, signs and markers manifest (express, reveal) themselves and (ii) changes in how disruptions are perceived (experienced, interpreted) subjectively, interpersonally and academically (two steps process).
Symptom expression can alternate within the B=L=C (“oneness”), B=C (”body-(of)-consciousness”; experiencing oneself), L=C (“phenomena”) and C (“meta-consciousness”) regions.
For example, manifestations of anxiety (fear), despair (pain) or anger (aggression) as “symptoms” can change among being (i) private (unobserved) behaviors (acts) (e.g. auto (“self”) soothing / harm, object destruction); (ii) biophysical bodily experiences) (e.g. internal distress, arousal, HBP); (iii) distortions of perception, cognition and ideation (e.g. dissociative disorientation / derealization / depersonalization, hallucinations, reality testing) and (iv) distortions of self-image / schema, defense mechanisms (e.g. “self-”hate”, denial, repression, suppression, reaction formation, fragmentation, idealization / devaluation).
Sign expression can alternate within the B=L=C=P (“mutuality”), B=C=P (“translocality”), L=C=P (“collective consciousness”) and C=P “ipsocentric mirroring”) regions.
For example, manifestations of anxiety (fear), despair (pain) or anger (aggression) as “signs” can change among being (i) publicly observable in-person behaviors (e.g. panic attack, phobic behaviors, depressed level of psychomotor activity , violations / violence); (ii) publicly known remote / virtual acts via phone, video, social media, news (e.g. crisis / suicide hotlines, pleas for help, threats / violence); (iii) formation of alternative “consensual reality” (e.g. psychosis, deception, idiosyncratic political / social / group ideology) and (iv) intersubjective / relational misattunment (e.g. ruptures of mentalization / intimacy / reciprocity / mutuality, microaggression, validation / invalidation).
Marker expression can alternate within the B=L=P (“corporeality”), B=P (“body-(of)-person”) and L=P (“locality”) regions.
For example, manifestations of anxiety (fear), despair (pain) or anger (aggression) as “markers” can change among being manifested in (i) unconscious facial expressions, body language, tonality of voice / speech (ii) changes of one’s perceptions by others as “anxious”, depressed”, “angry / aggressive” and (iii) association of one’s location with anxiety, fear, distress, anger or aggression leading to related dynamics of interpersonal / societal desirability, group membership, responses / preferences by others, career options / offers (location-based bias, stigma, stereotypes, prejudice).
Furthermore, expression and relative position of symptoms, signs and markers correspond to their perspectival position – how psychopathological i-states (p-i-states) are perceived (experienced and interpreted) subjectively, interpersonally and academically at a particular spatiotemporal location (Table P-3 below).
| SUBJECTIVE | INTERPERSONAL | ACADEMIC | |||||||
| ONE IS AWARE
OF IT |
CONSIDERED DISRUPTION | CONSIDERED PATHOLOGY | PERCEIVED BY OTHERS | CONSIDERED DISRUPTION | CONSIDERED PATHOLOGY | MEASURABLE | MARKER OF DISRUPTION | MARKER OF PATHOLOGY | |
| I-STATE (1) | Y | Y | SYMPTOM | N | – | – | N | – | – |
| I-STATE (2) | Y | Y/N | Y/N | Y | Y | SIGN | Y | Y/N | Y/N |
| I-STATE (3) | N | – | – | Y/N | Y/N | Y/N | Y | Y | MARKER |
(Y=Yes; N=No)
Table P-3 Psychopathology and perspectival position of i-states
A symptom is a private i-state, unobservable to others, experienced by one as a disruption of the here-now and considered to be a signifier of psychopathology (illness, disorder). Subjectively, one’s experience of a given p-i-state as a “symptom” can change when the degree of one’s awareness of it is modified (repression, suppression, distraction, denial, compartmentalization, etc.) and / or when it is not considered to be a disruption or a manifestation of psychopathology (re-framing, normalizing).
For example, anxiety (fear), despair (pain), anger (aggression) or ego-dystonic thoughts and desires as “symptoms” may be experienced with varying degrees of awareness (attention) or may come to be perceived as adaptive (not a “disruption”) or healthy (not “psychopathological”).
A sign is a public i-state perceived interpersonally as a disruption and a signifier of psychopathology. It may or may not be perceived as such subjectively or academically. Interpersonal perception of a p-i-state as a “sign” can change when it is perceived as a natural (non-disruptive) and / or normal (non-pathological) i-state in the here-now.
For example, a public expression of one’s thoughts, desires, feelings, sexual orientation, gender identity or any “non-conforming” i-state may be normalized from being perceived interpersonally as a psychopathological “disruption” (disorder) to being normatively acceptable, healthy and adaptive.
A marker is an i-state considered academically to be a disruption and a signifier of psychopathology. It is outside of one’s awareness and may or may not be experienced or considered a disruption or psychopathology interpersonally. Academic perception of a p-i-state as a “marker” is typically location and time specific (spatiotemporal) and changes based on academic perspective / framework / zeitgeist and conceptual / theoretical / empirical progress of academic understanding (knowledge) of biological, behavioral and interpersonal / relational correlates of psychopathology. For example, multiple diagnoses and markers (“criteria”) of psychopathology are being removed from and / or added to each subsequent edition or revision of the national (DSM) and international (ICD) classification systems of “mental disorders”, reflecting both academic / scientific progress and ever-expanding proliferation of diagnostic categories of psychopathology in the medical “marketplace”[6]
Changes in the disruptive relation to one’s health and resilience
Transformations of psychopathology are embedded and need to be contextualized within a particular understanding (model) of health, resilience and change.
Psychological health is not just an absence of psychopathology. It is an autonomous aspect of one’s uniqueness, a range of i-states involving adaptation, actualization and realization, in which one is at one’s best (optimal, ideal, desired) level of psychological functioning, subjectively, interpersonally and academically / scientifically.
Adaptation, actualization, realization
Adaptation (survival) typically refers to one’s ability to function as an autonomous, agentic, competent and productive member of one’s community without a need for ongoing assistance from others or societal institutions. One is able to secure (“to have”) adequate shelter, food, self-care, health, education, income, relationships required for an independent adaptive functioning.
Actualization (exploration, growth, mastery) refers to one’s pursuit of one’s own desires and inherent potential to reach (“to become”) one’s best and fullest at an optimal level conceivable (imaginable) to one and others.
Realization (transcendence, compassion, generativity) refers to one’s capacity to dedicate one’s life to others. Adaptation (“having / doing”, survival), actualization (“becoming”, progress) have been accomplished and are now transcended towards transubjectivity (interdependence, mutuality) of love and care (compassion) for and among others.
Correspondingly, ontological health (the intersection of adaptation, actualization and realization) is a formation of i-states in which one’s biophysicality (BODY), consciousness (EXPERIENCE), spatiotemporal (sensory / semiotic) space (LOCATION) and interpersonal / societal markers (PERSON) are at the best (optimal, ideal, desired) level of resilience, well-being, insight (awareness, wisdom), performance and transubjectivity (compassion, love) (see Graph P-4 below)
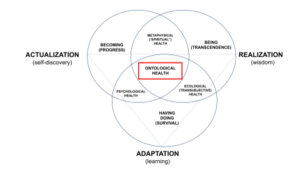
Graph P-4 Psychopathology and Health
Psychopathology is typically conceptualized as a problem (disorder, impairment, dysregulation) of adaptive functioning (adaptation). However, within the expanded Adaptation-Actualization-Realization (AAR) model, the same problem may not be considered to be a disruption or psychopathology of actualization or realization. For example, anxiety, despair or anger may be dysfunctional in terms of adaptation (survival) but, at the same time, be growth promoting in terms of one’s actualization (change). Similarly, renunciation (sacrifice) of one’s own desires, likely contrary to functional adaptation and actualization, can enhance one’s compassion (care), transubjectivity and ontological health (resilience) in a movement towards realization (transcendence). Correspondingly, ipsocentric pursuit of power (aggression) may not be conducive to realization (transcendence, ontological health) but be functionally adaptive (survival) and promote actualization (desires, growth).
Changes in the disruptive relation to one’s health and resilience involve shifts in how symptoms, signs and markers are perceived (experienced, interpreted) in relation to adaptation, actualization and realization whereby a disruption deemed psychopathological within one aspect of health may be health promoting within another. For instance, many common problems (disruptions) of adaptation (survival) (e.g. anxiety, despair, anger, dis-associations) may signal a unacknowledged need for a change towards aspirational actualization (lifestyle, career, relational) or transcendent realization (spirituality, generativity, transubjectivity, compassion, care).
Treatment – biological, psychological, systemic
Treatment is a sequence of interpersonal and intersubjective transactions whereby one (patient, recipient) is engaged with others (doctors, therapists) in the process of modifying (curing, healing) aspects of one’s uniqueness deemed to be a psychopathological disruption (p-i-states). Treatment can involve one or multiple regions within the four registers of uniqueness and focus on any aspect of (i) one’s body (biophysicality, appearance, behavior) (B); (ii) one’s consciousness (attention, awareness, ideation) (C); (iii) sensory / semantic context of one’s location (stressors) (L) and (iv) markers of one’s societal / interpersonal position (status) (P).
Biological, psychological, systemic and alternative approaches
Typical treatment approaches involve a combination of biological, psychological and systemic interventions. Although most treatment modalities aim to address all aspects of one’s uniqueness, biological interventions focus primarily on biophysicality and homeostatic regulation and involve direct manipulation of activity of the brain and nervous system (e.g. psychopharmacology, TMS, ECT). Psychological interventions are focused mainly on one’s consciousness, intersubjectivity (e.g. psychodynamic therapy, psychoanalysis) and interpersonal behavior (e.g. cognitive-behavioral / interpersonal therapy, skills training). Systemic interventions are focused on stressors, adversities and challenges within the sensory / semantic context of one’s location (natural, geopolitical, societal, family, relational) and involve a combination of environmental / societal / interpersonal modifications and skills training (e.g. politics, charity, health care, social activism, social media, education, family / systems therapy) and various types of stress management / resilience trainings.
Most modern treatment approaches draw extensively from ancient traditions of healing and wellness (traditional medicine) and perennial wisdom of health and self-transformation (e.g. Yoga, Buddhism).
[1] Siddhartha Gautama, (ca 567 – 413 B.C.E). Four Truths
[2] diathesis, stressors, adversities, trauma
[3] molecular, cellular and neural binding, sensorimotor coordination, coherence (unity, cohesion) of attention, awareness, perception, cognition, consciousness, homeostatic equilibrium, associative memory and learning, intelligence, executive functions, language and social / interpersonal behavior
[4] natural, adaptive, normative, expected
[5] Some of the most fundamental trajectories of transformation involve changes in (i) the ratio between ideation (thinking, imagining, remembering) and awareness of one’s sensations and (ii) transitions between awareness of here-now (being) vs awareness of elsewhere-then (remembering / planning) vs dissociations / psychosis / delirium / dementia
[6] Considered by many to be a reflection of progressive objectivization (monetization) of human experience in the context of individual anomie / otherness / alterity within the contemporary global culture.