The physical world (universe) does not get “ill” or have “symptoms”, it is normal (“healthy”) as it is. Life, however, with survival, adaptation and learning (memory) at its core, brings in the possibility and the inevitability of dysfunction, illness (disorder) and demise (death). Physical disorders (illness, dysfunction) are part of life and death. Psychopathology, an aspect of life, has emerged along with and is predicated on the evolution of senses, awareness, consciousness, ideation (meaning, interpretation, remembering) and, eventually, systems of signs and languages (culture).
Psychopathology is an aspect of uniqueness (p-i-state)[1] which is perceived (experienced) by one and / or others as a breakdown (disruption, failure) of a natural (adaptive, healthy, normal) i-state within the here-and-now of one’s location and attributed to a (known) mental disorder (syndrome, illness).
It is a neurocognitive impairment (dysregulation) of one’s body and consciousness, a disruption or absence of a desired or expected natural (healthy) neurocognitive function and / or related behavior that is (i) experienced by one and / or observed by others; (ii) associated with a degree of distress ( pain, suffering, discomfort), (iii) attributed to psychopathology and (iv) studied, researched academically (syndromes with hypothesized etiology, course, prognosis and cure) and diagnosed (identified, labeled, cataloged) as specific “mental disease”. Perception and interpretation of an i-state as “psychopathological” (p-i-state) vs “normal” “healthy” “adaptive” (i-state) may vary both among and within the subjective, interpersonal and academic perspectival points of view.
Psychopathology manifests as symptoms, signs and markers.
Most broadly, symptoms are experienced and defined subjectively and private (unobserved) interpersonally. Signs are experienced and defined both subjectively and interpersonally. Markers are outside of one’s awareness (nonconscious), observable (measurable) and defined and studied academically, based on self-reports, observation and research data (See Graph PP-SIO below)
For any i-state to be considered a symptom, sign or marker (p-i-state), it has to be (i) experienced (represented in awareness) by one (symptoms, signs) and / or by others (signs, markers) as a disruption (dysregulation, failure, absence, violation) and (ii) interpreted to be an indication of psychopathology. Many disruptions are not considered to be “psychopathological” and are often referred to as “problems” (errors, concerns, trouble, difficulty, etc.) and definitions of “psychopathology” vary within and between the subjective, interpersonal and academic perspectives.
Subjectively, for an i-state to become a symptom it has to be (i) represented in one’s awareness (attention); (ii) experienced as a disruption and (iii) interpreted to be an indication of psychopathology.
Interpersonally, for an i-state to become a sign it has to be (i) observed by others; (ii) perceived as a disruption and (iii) interpreted as an expression of psychopathology. Academically, for an i-state to become a marker of psychopathology it has to be (i) observable (measurable); (ii) a disruption and (iii) an aspect of a diagnostic syndrome.
Since perception and interpretation of an i-state as a “disruption” or “psychopathology” (p-i-state) vs “normal” “healthy” “adaptive” (i-state) may vary among the subjective, interpersonal and academic perspectives, the uniqueness of individual “psychopathology” can manifest in multiple ways (See Table PP-SIA below)
|
|
SUBJECTIVE |
INTERPERSONAL |
ACADEMIC |
||||||
|
|
ONE IS AWAREOF IT |
CONSIDERED DISRUPTION |
CONSIDERED PATHOLOGY |
PERCEIVED BY OTHERS |
CONSIDERED DISRUPTION |
CONSIDERED PATHOLOGY |
MEASURABLE |
MARKER OF DISRUPTION |
MARKER OF PATHOLOGY |
SYMPTOMS |
Y |
Y |
Y |
N |
– |
– |
N |
– |
– |
SIGNS |
Y |
Y/N |
Y/N |
Y |
Y |
Y |
Y |
Y/N |
Y/N |
MARKERS |
N |
– |
– |
Y/N |
Y/N |
Y/N |
Y |
Y |
Y |
Table PP-SIA – Perspectival aspects of psychopathology
Symptoms, signs and markers form a matrix of at least eleven distinct manifestations (p-i-states) of psychopathology based on (i) one’s epigenetic / developmental trajectory of associative integration, homeostatic / relational regulation and the formation of the “I”; (ii) the register of uniqueness in which a disruption occurs[2] and (iii) the magnitude (severity) of the disruption[3] and (See Graph IS-P below):
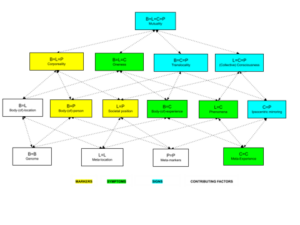
Graph IS-P – I-STATE and Psychopathology
Symptoms – regions B/L/C, B/C, L/C, C
Fundamentally, a symptom is an aspect of one’s uniqueness that (i) disrupts the spatiotemporal here and now of one’s location and (ii) interferes with (dysregulates) one’s ontological health[4]. It is an i-state at the interface of one’s consciousness (C), body (B) and location (L) where events in one’s body and consciousness (sensations, feelings, awareness, ideation) (i) are incongruent with or violate the immediate sensory / semiotic here-and-now and (ii) are interpreted to be a problem, impairment, dysregulation and (iii) are deemed to be a manifestation (sign) of a dis-ease (sickness, illness).
The “incongruence” with the immediate here-now is a function of neurocognitive autonomy of the nervous system and human consciousness – an evolutionary capacity to function independently (beyond) the immediate physical / sensory context and to select or create (add) idiosyncratic meanings (signification, signifiers) to the spatiotemporal (sensory, semantic) location based on memory, learning or ideation. To interpret an i-state to be a problem (impairment, dysregulation) means to compare it to other i-state(s) (actual or imagined) and deem it to be inferior, undesirable (unwanted) and / or a “sign” associated with a concept or a theory (private and / or public) of an “illness” (psychopathology).
The neurocognitive capacity to alter or to transcend the sensory / semiotic here and now of one’s location is the evolutionary aspect of consciousness involving memory, learning and ideation and is inherently adaptive and healthy. However, if it is experienced and interpreted as a problem, impairment, dysregulation (disruption) or a manifestation (sign) of a dis-ease (sickness, illness), it may become a symptom. Most, if not all, events (experiences) beyond the here and now, or some of their aspects, may be adaptive (healthy). Anxiety, fear, anger, shame, guilt, dissociations, hallucinations, idiosyncratic / nonlinear ideation, confusion, disorientation have a place in human experience. They become “symptoms” when they are deemed (experienced, interpreted) to be a problem and a marker of “psychopathology”.
A symptom may be aversive (distressing) (e.g. “anxiety”) or pleasurable (enjoyable) (e.g. “perversion”, “addiction”). Although almost any i-state can be experienced by one (subjectively) as “aversive” or a “problem” or believed to be a “symptom” of an impairment (disease, illness), not all aversive or problematic i-states are “symptoms” or “signs” of psychopathology. Actually, many aversive and / or unwanted i-states are or can be beneficial and not considered to be markers of psychopathology. Furthermore, being present in the here and now is not only an experience, it is also an embrace of and participation (taking part) in the here and now. Consequently, psychopathology and health are associated with the capacity to be fully present, aware and participation in the relevant aspects of the here-now.
Symptoms are experienced and they are experiences. As an experience, a symptom involves (i) an experiencing agent (subject) – the “I” (sensorimotor, sensoriaffective, ideational or communicative)[5]; (ii) modality – a specific sensory or ideational process (seeing, hearing, feeling, thinking, remembering, imagining) through which the symptom becomes an experience and (iii) the content of what is experienced – a specific biophysical, semiotic / semantic, experiential or interpersonal / societal event / entity (e.g. snake phobia = fear (feeling) of snakes (elongated reptiles).
The experience of a symptom is predicated on the formation of the experiencing “I” (subject, agent). How the “I” is formed (arises) contributes to the experience and the formation of the symptom which can take place within one or between two modalities (modes). Experiencing the symptom within the same modality has to do with increased capacity (readiness) to extend (add beyond) the here and now whereas experiencing it between different (other) modalities one is more likely to interpret it to be a problem (impairment) and / or a sign of psychopathology.
Symptoms are typically experienced (subjective perspective) as elemental (singular, unified) and usually understood (the academic perspective) as composite compounds and contextual (among other events and relations) within one’s UNIQUENESS (being, life). For instance, the symptom experienced as “anxiety is usually a compound which may include excessive worry (apprehensive expectation), perspiration, trembling, muscle tension, shortness of breath, etc. Similarly, the symptom of “depression” may consist of sadness, hopelessness, anhedonia, irritability, lethargy and worthlessness. In the academic discourse, configurations of symptoms and signs with shared etiology, mechanism and prognosis become diagnostic syndromes.
Most symptoms are typically formed within the B/L/C region but there are also specific ones associated mainly with regions B/C, L/C and C (see Table PS below).
Symptoms within the B/L/C region (oneness, qualia) involve tri-modal, private (unobserved) events formed at the intersection of one’s body (biophysicality, behavior, appearance), location (coordinates, semiotic space) and consciousness (sensations, awareness, ideation). Prototypical B/L/C symptoms and their compound components include most dysregulations of private (unobserved) behaviors (avoidance, isolation, self-harm, inhibitions, rituals, compulsions, addictions). The B/L/C symptoms are embedded within and involve one’s location.
Symptoms within the B/C region (body-(of)-consciousness) involve bi-modal, private (unobserved) events formed at the intersection of one’s body (biophysicality) and consciousness (sensations, awareness, ideation). Prototypical B/C symptoms and their compound components include i-states associated with neurocognitive (endogenous or “psychosomatic”) dysregulation of arousal / activation (e.g. lethargy, insomnia, restlessness, inhibitions), mood (e.g. manic / depressed mood, anhedonia), affects (irritability, anger, stress, panic, euphoria), cognition (e.g. attention / concentration, memory), somatization (e.g. headache, gastrointestinal, cardiovascular) and body image (e.g. body dysmorphic disorder, anorexia). The B/C symptoms are independent of one’s location.
Symptoms within the L/C region (phenomena) are bi-modal events at the interface of semiotic / sensory space (horizon) of the location and one’s consciousness (sensations, awareness, ideation) involved in the formation of a “reality” (properties of shape, color, up / down, left / right); boundaries and distinctions of me / you, here / there, close / far); spatiotemporal orientation and regulation of position, time, place).
Prototypical L/C symptoms include any phenomenal dysregulation of spatiotemporal orientation (disorientation) often associated with delirium, psychosis, intoxication, derealization or cognitive confusion.
Symptoms within the C region (meta-consciousness) are uni-modal i-states involving consciousness of one’s own consciousness (sensations, awareness, ideation about own sensations, awareness, ideation).
Prototypical C symptoms include dysregulation of self-awareness / self-consciousness – awareness of and ideation about own consciousness and typically involve distressing (ego-dystonic) fragmentation / distortion / devaluation of own experience (self-loathing, ruminative self-absorption, identity confusion, depersonalization, disorientation about oneself)
|
|
PROTOTYPICAL SYMPTOMS |
|
B/L/C |
Dysregulation of private (unobserved) behaviors (avoidance, self-harm, inhibitions, rituals, compulsions, addictive) |
|
B/C |
Dysregulation of homeostatic biophysicality (sensations, mood / affect, activation / arousal / inhibition, psychosomatic / somatization) |
|
L/C |
Dysregulation of perception and cognition of spatiotemporal “reality” of one’s location (disorientation / confusion / derealization / depersonalization / thought disorder, hallucinations) |
|
C |
Dysregulation of awareness of and ideation about own experience (self-awareness / self-consciousness, identity). Fragmentation / distortion / idealization / devaluation of own experience. |
Table PS – Prototypical Symptoms
Signs – regions B/L/C/P, B/C/P, L/C/P, C/P
Sign is an i-state experienced both by one and others as (i) being beyond the sensory / semiotic here-and-now and (ii) deemed by others to be a disruption and (iii) a marker of psychopathology. Signs are observed by others, distinct from private symptoms and inherently intersubjective. Private (unobserved) behavioral symptoms become signs when an observer is aware of them. Signs may or may not be considered a disruption and / or aspect (markers) of psychopathology subjectively and academically.
Most signs are typically formed within the B/L/C/P region but there are also specific ones associated mainly with regions B/C/P, L/C/P and C/P (see Table PSi below)
Signs of psychopathology within the B/L/C/P region (mutuality) are public four-modal i-states experienced by one and others as misattuned with (beyond / outside of) the here-and-now and deemed to be disruption and an aspect of psychopathology interpersonally but not necessarily subjectively and / or academically. One’s experience of the i-state is congruent with perception of it by others in that one is aware of it. Prototypical B/L/C/P manifestations include (i) public violation of norms or expectations (e.g. inappropriate or criminal behavior); (ii) failed action (e.g. accidents, failure to execute) and (iii) any observable dysregulation of behavior or appearance (e.g. parapraxes, excessive inhibition / activation, dissociation)
Signs of psychopathology within the B/C/P region (translocality) are public tri-modal i-states (i) autonomous of or (ii) incongruent with one’s and / or others’ location and deemed to be markers of psychopathology. Prototypical B/C/P signs are remote (virtual) or beyond (outside) of just one spatiotemporal location and, correspondingly to the B/L/C/P ones, may include (i) public violation of norms or expectations (e.g. virtual / cybercrime), (ii) failed action (news, telecommunication, social media, sports); (iii) observable dysregulation of behavior or appearance associated with spatiotemporal (dis)location (e.g. trans, dissociation, flashbacks, altered states) and (iv) construction, experience and interpretation of a spatiotemporal location that are mutually incongruent across the subjective, interpersonal, academic perspectives.
Signs of psychopathology within the L/C/P region (collective consciousness) are public tri- modal i-states (i) incongruous with the shared (collective) consciousness of a “reality” and (ii) deemed to be markers of psychopathology. Prototypical L/C/P signs include violations of or failure to adhere to the shared collective consciousness of a reality (e.g. deception, biophysical (behavioral) masquerade, cognitive disorientation, psychosis, dis-association, maladaptive otherness, confusion about collective identity). Nonconformism, political / social action, art challenging the collective consciousness are typically not considered a sign of psychopathology unless deemed to be so by one or others within the subjective, interpersonal or academic point of view.
Signs of psychopathology within the C/P region (ipsocentric mirroring) are bi-modal i-states (i) involving a violation or failure of intersubjective relatedness and (ii) deemed, subjectively, interpersonally or academically, to be markers of psychopathology.
Prototypical C/P manifestations include mutual misrepresentations, stereotyping / profiling, bias, idealization / devaluation / distortion, interpersonal (personality) conflicts, delusions resulting in dysregulation of relatedness.
|
|
PROTOTYPICAL SIGNS |
|
B/L/C/P |
Dysregulation of observable location-specific public behavior (norms, expectations, crime, accidents, breakdowns, failures) |
|
B/C/P |
Remote (virtual) dysregulation of observable interpersonal behavior (norms, expectation, failed action, accidents) |
|
L/C/P |
Dysregulation of shared collective consciousness (representation, interpretation) of consensual reality (psychosis, deception) |
|
C/P |
Dysregulation of intersubjective relatedness (mentalization, projective identification, intimacy, empathy) |
Table PSi – Prototypical Signs
Markers – regions B/L/P; B/P, L/P
A marker is a behavior or appearance, outside of one’s awareness (nonconscious), interpreted academically (i) as being beyond the sensory / semiotic here-and-now (disruption) and (ii) a marker of known psychopathology. They are nonconscious, observable (measurable, public) and distinct from symptoms and signs. One is unaware of markers or of their meaning for others and is often reluctant / resistant to acknowledge them. Markers are used, academically, to infer (mark, diagnose) presence of psychopathology in others, are distinctly contextual and subject to the zeitgeist of the time.
Markers are typically formed within the B/L/P, B/P and L/P regions and involve dysregulation of (i) observable behaviors and appearance, (ii) measurable internal biophysicality and (iii) location, respectively (see Table PM below)
Markers within the B/L/P region (corporeality) are public tri-modal i-states (i) outside of one’s awareness (or misunderstood); (ii) incongruous with or a disruption (violation) of the consensual and expected (normative) “reality” of the here-and-now of others and (iii) interpreted academically to be indicative of psychopathology. They are observable behaviors, including speech and appearance and may involve behaviors that one is unaware of (nonconscious) or interprets differently than others do (e.g. “ego-syntonic”) and may include any behavior experienced by others as deviant, concerning, abnormal, bizarre, irrational, inappropriate, threatening, etc. including non-conscious bodily and facial displays (facial expressions, grimacing / tics, body postures / gestures / appearance, automatic / habitual movement, mannerisms) or speech that are incongruous with or in violation of the consensual “reality” of the here and now and experienced by others as odd, disgusting, threatening, alien, random, irrational, inappropriate and an indicator of psychopathology.
Markers within the B/P region (body-(of)-person) are any bi-modal observable and measurable dysregulations (disruptions) of typical (healthy, normal) homeostasis of one’s biophysicality deemed to be markers of psychopathology (p-i-state). They may include any measures of internal biophysical processes (stress, arousal, heart rate, electrodermal activity, sleep / wake rhythms, metabolism) or any biophysical marker (size, temperament, gender, race, ethnicity) associated academically with known diagnostic syndromes.
Markers with the L/P region are bi-modal i-states involving societal / interpersonal signification of one’s location as a non-conscious but observable and measurable disruption of the public (semiotic) context of the here-and-now deemed to be a marker of known psychopathology (institutional care facility, trespassing, dislocation, homelessness, stereotyping / bias).
|
|
PROTOTYPICAL MARKERS |
|
B/L/P |
Dysregulation of observable / measurable but nonconscious behavior (deviant, threatening, inappropriate, alien, random) |
|
B/P |
Dysregulation of measurable homeostatic biophysicality (stress, arousal, heart rate, sleep / wake rhythms, metabolism) |
|
L/P |
Dysregulation of one’s spatiotemporal / interpersonal / societal position (location) and its semiotic context |
Table PM – Prototypical Markers
Contributing factors – regions B/L, B, L, P
Contributing factors are associated with the formation of symptoms, signs and markers as i-states outside of one’s awareness, some of which can be observable and studied academically. Most of them function within the B and B/L regions, several others in the L and P regions.
Contributing factors within the B/L region (body-(of)-location) are bi-modal i-states associated with embodying spatiotemporality. B/L i-states include body temperature, metabolism, biophysical processes, internal activation / pace / rhythm, spatiotemporal coordination of private aspects of one’s position, posture, movement, reflexes / habits / tics / mannerisms. Psychopathology of the B/L region may include homeostatic / biophysical dysregulation (hormonal, neurotransmission, metabolic) – jet lag, altitude sickness, new diet, environmental stress (noise, pollution, light, sleep-wake cycle).
Contributing factors within the B region (genome) are uni-modal (nonconscious, unobservable directly) i-states within one’s genome autonomous of the effects of location, consciousness and societal / interpersonal markers (aging, randomness). They may involve changes in the architecture, sequence or functioning of one’s genes (mutation, duplication, rearrangement) which may contribute to the formation of psychopathology.
Contributing factors within the L region (meta-location) are autonomous, uni-modal i-states encompassing the totality of signs, symbols, narratives within the location about the location itself, independently of one’s biophysicality, experience, and one’s societal / interpersonal markers. It is how a location refers to itself – collective consciousness of others about the location itself – the location in the minds of others (representation). The i-states within the L region may contribute to the formation of pathogenic (i) experience (sensations, awareness, ideation e.g. identity, self (image / schema), feelings, beliefs); (ii) biophysicality, behavior and appearance (resilience, stress, activation, NVS (pain), PVS (pleasure) and (iii) interpersonal / societal markers (positive / negative bias, stereotyping / profiling, violence vs acceptance)
Contributing factors within the P region are autonomous, uni-modal i-states encompassing societal / interpersonal markers (opinions, beliefs) about one’s markers, (memories, records, products) which may have pathogenic effects (“stressor”) on one’s body, consciousness and location.
|
|
PROTOTYPICAL CONTRIBUTING FACTORS |
|
B/L |
Pathogenic homeostatic / biophysical dysregulation of the body-(of)-location (B/L) (embodying spatiotemporality) |
|
B |
Pathogenic biophysical changes (random, time-related) within one’s genome (mutation, duplication) |
|
L |
Pathogenic signs, symbols, narratives within the location about the location itself (self-representation) |
|
P |
Pathogenic societal / interpersonal markers (opinions, beliefs) about one’s markers, (memories, records, products). |
Table PCF – Prototypical Contributing Factors
[1] “p-i-state” = psychopathological i-state
[2] See sections other posts
[3] ibid
[4] ibid
[5] ibid